

The impact of gang violence on a youth’s risk for death or injury is tremendous. Prevention of complex societal problems, such as gang violence, requires a substantial effort and commitment from many sectors and disciplines. Nurses are uniquely positioned to help lead such efforts. Understanding the public health perspective to gang violence may be an important tool for nurses attempting to prevent this problem. The public health approach has four key components: defining and monitoring the problem; identifying risk, protective, and promoting factors; developing and evaluating interventions; and dissemination. This article outlines these components, current research on gang violence, and concludes by summarizing critical challenges for nurses to consider as they contribute to public health initiatives to prevent gang violence.
Key Words: gang, gang violence, youth, public health, nursing
From 2002 to 2006, gangs were responsible for approximately 20% of homicides in the 88 largest United States (US) cities. Many health providers might not think they would see the words “gang violence” and “public health” in the same sentence. However, nurses who work in emergency rooms, schools, local public health agencies, and health clinics located in communities with high levels of gang activity likely have daily reminders that gang violence and public health do intersect. In reaction to research showing an ‘epidemic’ of gang violence in many urban areas (Hutson, Anglin, Kyriacou, Hart, & Spears, 1995), the nursing community identified gang-involved youth as a vulnerable population in need of services that can help prevent gang violence and improve the health and well-being of this population (Sanders, Schneiderman, Loken, Lankenau, & Bloom, 2009).
From 2002 to 2006, gangs were responsible for approximately 20% of homicides in the 88 largest United States (US) cities (Pyrooz, 2011). Preventing gang affiliation and the formation of gangs might significantly reduce gang-related violence. The emergence and persistence of gangs is thought to be a byproduct of societal problems, such as social, economic, and educational disparities (Howell, 2012). Youth may become involved with gangs to gain a sense of control and power over these social disparities and to have a sense of camaraderie with others, especially if they lack strong connections with parents, other family members, and peers (Howell, 2012). Instead of social connection, these youth become further isolated from more positive social members of society and social, religious, and educational institutions, such as schools, faith-based institutions, and social services (Klein & Maxson, 2006). Youth may become involved with gangs to gain a sense of control and power over these social disparities and to have a sense of camaraderie with others... Sometimes, it is not until youth are seriously injured from gang violence that they get re-connected to more positive social institutions through the help of professionals in the health care sector. Therefore, in this capacity nurses are uniquely positioned to help lead gang violence prevention efforts and improve the health and well-being of this vulnerable population.
Many nurses have the desire to help youth involved in gangs, but may not know the best way to address this problem within their occupational role. This article outlines one method, the public health approach, for understanding and preventing gang violence. Specifically, we discuss why a public health approach is useful to preventing gang violence; how each component of the public health approach can be applied to prevent gang involvement, gang violence, and other gang activity; and how nurses can use their role to support public health strategies intended to reduce gang violence.
A Public Health Perspective on Gang Violence Prevention
Traditionally, the field of criminal justice has studied gang violence (Klein & Maxson, 2006). While many sociologists have also explored this problem (Klein & Maxson, 2006), in the past two decades, additional health-oriented fields, such as nursing, medicine, and psychology, have increasingly studied gang violence. Each discipline and sector contributes a unique perspective on gang violence. However, collaboration across multiple disciplines and sectors is necessary to develop a more comprehensive understanding of gang violence. The book, Changing Course: Preventing Gang Membership (2013), represents one such collaboration between criminal justice and public health. This book offers a multidisciplinary perspective on gang violence prevention, combining knowledge to provide new insight into potential solutions to prevent gang joining.
...collaboration across multiple disciplines and sectors is necessary to develop a more comprehensive understanding of gang violence. The public health approach encourages basic research into the nature of a problem and the application of these findings to develop, implement, evaluate, and disseminate specific prevention strategies. This approach also encourages collective action, which includes the participation and collaboration of many sectors of a community (e.g., law enforcement, health, and education). Public health focuses on primary prevention, which provides a complement to the usual interventions for gang-involved youth (i.e., incarceration/arrest, and treatment of violence-related injuries) (CDC, 2009). Primary prevention is aimed at preventing the development of aggressive or violent behaviors before they begin and helping to set positive developmental and behavioral trajectories for youth.
The public health approach to violence prevention involves a four-step process that is grounded in the scientific method (Dahlberg & Krug, 2002; Haegerich, Mercy, & Weiss, 2013).
- The first step in the public health approach is describing and monitoring the problem, and tracking trends.
- The second step includes identifying factors that increase risk (i.e., risk factors); factors that protect against or buffer risk (i.e., protective factors); and factors that promote positive behaviors (i.e., promotive factors).
- The third step includes the development and evaluation of prevention policies, strategies, and programs that are intended to reduce risk factors and increase protective and promotive factors.
- The final step emphasizes the broad dissemination and implementation of the prevention policies, strategies, and programs.
The public health approach has been widely promoted by the Centers for Disease Control and Prevention (CDC) to address a variety of types of violence, including youth violence, child maltreatment, and intimate partner violence. In addition, the public health sector has had great success in using this model to target other complex health behaviors, such as tobacco use, motor vehicle crashes, and coronary heart disease (Rosenberg, O'Carroll, & Powell, 1992).
Define and Monitor the Problem
The first step in the public health approach is to define and monitor the problem. Public health offers a unique perspective in regard to this step in the scientific method because this approach is not just focused on the health of individuals; rather it focuses on societal or population-based problems. Often information used to define and monitor health problems is called public health surveillance data. These data are used to explore how health problems are distributed across populations to provide insight on where to focus prevention strategies, as well as how they might need to be adapted to maximize positive impact.
Since there is not a uniform definition of a “gang,” surveillance of gang violence is often very challenging. Public health researchers typically begin surveillance efforts by establishing a case definition of a health problem that they intend to monitor (Lee, Thacker, & Louis, 2010). Case definitions need to be specific enough to ensure that the data elements are consistent and comparable over time. Since there is not a uniform definition of a “gang,” surveillance of gang violence is often very challenging (Esbensen, Winfree, He, & Taylor, 2001; Klein & Maxson, 2006). These varying definitions can lead to problems interpreting data. A broad definition of a “gang” may lead to an overestimate of the gang problem, whereas a more narrow definition may lead to an underestimate. In turn, these definitions may then impact resource allocation.
Incidents of health problems or persons with health conditions that meet the case definition are often called “cases” or case-patients. Researchers examine basic case counts to track health problems across populations. In addition, researchers often gather details to better understand the case characteristics, so that they can identify the “time, person, and place” associated with the public health problem. For example, The CDC's National Violent Death Reporting System (NVDRS) is a public health surveillance system that has collected information since 2003 on violent deaths, including gang-related homicides, across a number of states in the US. (CDC, 2007; Karch et al., 2012). This surveillance system regularly tracks new cases of gang homicides over time to identify ongoing trends and patterns. This system also provides case details with regard to place of death, such as the counts by states and cities, or the place of injury, such as street or residence. As far as the persons involved, the system captures demographic characteristics of both the victim and any known suspects. A recent study using NVDRS found that in five US cities—Los Angeles, Long Beach, Oakland, Newark, and Oklahoma City, gang-related homicides more commonly involved young adults and adolescents; racial and ethnic minorities; and males compared to other homicide types (CDC, 2012). Also, these gang-related homicides were often more likely to occur on a street and in afternoon/evening hours (CDC, 2012).
In 2011, the National Youth Gang Survey found that there were an estimated 29,900 gangs and 782,500 gang members throughout the 3,300 jurisdictions surveyed in the United States. Several other surveillance systems capture information important for understanding gang violence. The National Youth Gang Survey, funded by the Office of Juvenile Justice and Delinquency Prevention (OJJDP), is the only nationally representative survey on gang violence (Egley & Howell, 2013; "The National Gang Center," 2013a). This survey gathers data from more than 2,500 law enforcement agencies, including all police departments in cities of 50,000 or more, all suburban departments, and a random selection of rural and small city police and sheriffs’ departments (Egley & Howell, 2013). This survey asks each agency about gang activity, and estimates the number of gangs and gang members, the number of gang homicides, and other characteristics that describe the city’s gang problems (Egley & Howell, 2013). In 2011, the National Youth Gang Survey found that there were an estimated 29,900 gangs and 782,500 gang members throughout the 3,300 jurisdictions surveyed in the United States (Egley & Howell, 2013). In 2011, slightly fewer law enforcement jurisdictions reported gang activity than in 2010 and gang activity was mainly concentrated in highly populated areas (Egley & Howell, 2013).
There are also some surveillance systems that track the impact of gang violence in communities (e.g., injuries and violence victimization cases). For example, hospital-based injury surveillance systems that monitor gang-related injuries are often used to better understand non-fatal injuries related to gang violence in urban areas. In 2001, six Newark, New Jersey emergency departments participated in an assault-related surveillance project (Boyle & Hassett-Walker, 2008). When the victim-offender relationship was described in the assault, 14.5% of the assaults were found to involve gangs or group attacks (Boyle & Hassett-Walker, 2008). Nurses working in emergency departments or hospital settings looking to embark on gang violence prevention research and/or prevention initiatives might explore such hospital-based systems to better understand the magnitude and burden of gang violence in their communities.
Some elements of the health burden of gang violence may make up the bulk of one’s work, but are not currently captured by surveillance systems. Violence victimization is also an important indicator of the impact of gang violence. The CDC and OJJDP support the National Survey of Children’s Exposure to Violence (NatSCEV). This survey collects information on many forms of violence (i.e., 45 different kinds of violence, abuse, and victimization) in a nationally representative sample of 4,500 children, ages 17 and younger (Finkelhor, Turner, Ormrod, & Hamby, 2010). NatSCEV includes information on whether an assault involved a group of youth or a youth gang. Using this survey, it was estimated that 2.2% of children in the U.S. experienced a group or gang-related assault in 2008 (Finkelhor et al., 2010). Statistics from community surveys have important implications for school nurses, pediatric nurse practitioners, or other nurses who work in non-hospital-based settings. Nurses in these settings may see the physical injuries that do not result in a visit to an emergency departments or hospitalization, and they may need to care for children who suffer from the mental health consequences of gang violence. Some elements of the health burden of gang violence may make up the bulk of one’s work, but are not currently captured by surveillance systems.
Public health data systems also can capture information on behaviors that contribute to death and injury, such as gang involvement and gang-related activities. For example, the National Longitudinal Study of Adolescent Health (Add Health) includes a nationally representative sample of adolescents in grades 7-12 in the US. (Harris et al., 2009). In 1996, these adolescents were asked “Have you been initiated into a named gang?” Based on this question, it is estimated that 5% youth in the US reported that they had been initiated into a gang (Glesmann, Krisberg, & Marchionna, 2009).
The statistics presented in this section are meant to demonstrate the magnitude of the gang problem in the US. These statistics are however not without their limitations. For example, the “gangs” captured in NatSCEV include any peer group, the “gangs” in the National Youth Gang Survey exclude adult gangs, and the “gang” in NVDRS coding relies on definitions used by law enforcement agencies, which differ across jurisdictions. To address this problem, a group of gang researchers has collaborated to create a standardized definition (Klein & Maxson, 2006). They define gangs as “any durable, street-oriented youth group whose involvement in illegal activity is part of its group identity” (Klein & Maxson, 2006, p.6 ). This definition excludes motorcycle gangs, prison gangs, and other more traditionally adult groups, such as organized crime gangs. Until this definition is more widely adopted, definitional issues will be a limitation for gang research. To encourage use of this definition, a compilation of measurement tools have been developed for use in studying gang violence ("The Eurogang Project," 2013).
Identifying Risk, Protective, and Promotive Factors
The second step in the public health approach includes studying risk, protective, and promotive factors. Several models used in public health provide a framework to identify potential causes of health problems and to facilitate the development of prevention and intervention programs. Specifically, researchers have applied public health models, such as infectious disease models, social determinates of health models, and socio-ecological models, to better understand gang problems. This section will review these models and selected research that utilizes them
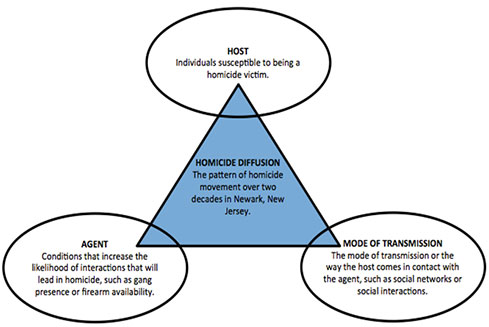
Racial segregation, economic disadvantage, and the movement of public housing complexes appeared to act as important agents in the movement of homicide over time.Infectious Disease Model. Typically, public health researchers use infectious disease models to show the relationship between a host, causative agents, and the mode of transmission of a disease. Using homicide as the “disease,” a recent study applied this model (see Figure) to examine if gangs and firearms were agents of homicide in Newark, New Jersey (Zeoli, Pizarro, Grady, & Melde, 2012). Zeoli et al. (2012) discovered that other agents appeared to be more important in the transmission of homicide. Racial segregation, economic disadvantage, and the movement of public housing complexes appeared to act as important agents in the movement of homicide over time. In addition, the study showed that gang homicides occurred in areas that already had high homicide levels, suggesting that gangs emerged out of these areas. Developing this better understanding of the potential causes of homicides in Newark had important implications for the design and targeting of prevention strategies. Specifically, Newark’s programs needed to focus on economic disadvantage and racial isolation.
Figure. Application of an Infectious Disease Model to Homicide (Zeoli et al., 2012)
Social Determinates of Health Model. In the social determinates of health model, elements of the community environment (e.g., socio-ecological context), such as income inequality, quality of schools in a community, low levels of trust among neighbors, and few safe places to exercise, are seen as shaping an individual’s living and working conditions.
Although sexual education is controversial in some school districts, it may be particularly important for schools with gang problems. These elements also shape his or her social and community networks, which in turn influences behavior and attitudes (Marmot, Friel, Bell, Houweling, & Taylor, 2008). This model can be useful for understanding societal problems, such as gang violence, which are highly impacted by the socio-ecological context where an individual lives. This model encourages research to examine structural issues, such as income inequality and demographic changes, instead of just focusing on characteristics of individuals (Marmot et al., 2008). Minnis et al. (2008) used a social determinates model to identify how the underlying social determinant of gang membership influences pregnancy through intermediate behavioral factors (e.g., contraceptive use, pregnancy intentions, and partnership characteristics). This study found that having a sexual partner who was involved in a gang was associated with an increased risk of pregnancy. It highlights the importance of addressing issues related to sexual education with gang-affiliated youth. Nurses who work in family planning clinics have the opportunity to screen their patients for involvement in gangs or relationships with gang-affiliated partners, and use this information to individualize the sexual education they provide. Although sexual education is controversial in some school districts, it may be particularly important for schools with gang problems.
...consistent predictors of joining a gang include: problem behaviors,... a youth’s experience of negative life events; and a youth’s attitudes toward delinquent behavior. Socio-Ecological Model. The third model, the socio-ecological model, is useful to explore the individual, relationship, community, and societal factors that affect gang involvement (Dahlberg & Krug, 2002). This model provides a framework for organizing risk and protective factors and also prevention and intervention strategies. At the individual level, the person’s psychological, behavioral, biological, and personal history factors are examined (Dahlberg & Krug, 2002). For example, in a review of 20 studies since 1990, Klein and Mason (2006) found that consistent predictors of joining a gang include: problem behaviors, such as reactivity, aggressiveness, and impulsivity; a youth’s experience of negative life events; and a youth’s attitudes toward delinquent behavior.
At the relationship level, the individual’s relationships to his or her peers, parents, and other close relationships are examined (Dahlberg & Krug, 2002). When youth are involved in gangs, their rates of participation in crimes and violence go above and beyond levels expected by their peers (even their delinquent non-gang peers) (Esbensen et al., 2001). An explanation for this finding is that the gang has an exaggerating influence on an individual’s negative behaviors, encouraging participation in violence and crime typically not engaged in without the peer influence. Having delinquent peer relationships is a consistently supported risk factor for gang membership (Klein & Maxson, 2006). Most studies also show support for the association of lack of parental supervision to gang membership (Klein & Maxson, 2006).
An explanation for this finding is that the gang has an exaggerating influence on an individual’s negative behaviors, encouraging participation in violence and crime typically not engaged in without the peer influence. At the community level, schools and neighborhood factors are examined, as well as the gangs themselves (Dahlberg & Krug, 2002). Klein and Maxson (2006) found inconclusive support for school and neighborhood influence on gang affiliation. Yet, relatively few studies have examined factors such as the presence of gangs in a youth’s school and/or a youth’s feelings of safety in school, so more research is needed to understand relationships between gang affiliation and risks at this level of the socio-ecological model. A much stronger literature base exists for examining the relationship of community level factors and the emergence of gangs. In this literature, city size, economic deprivation, social instability, racial/ethnic composition of the community, and poverty all were found to play a role in the emergence of gangs in a community (Klein & Maxson, 2006).
Finally, at the societal level, social and cultural norms and policies that maintain economic and social inequality among groups are examined (Dahlberg & Krug, 2002). Societal level risks and protective factors deserve more attention in the literature. While much of gang prevention efforts are aimed toward preventing gang involvement, interventions at the societal level may be able to prevent formation and persistence of the gangs themselves.
Developing and Evaluating Interventions
The first two steps of the public health approach provide contextual information needed to most appropriately target populations at risk for violence and factors that need addressed while planning interventions. In public health, intervention is often seen as involving a spectrum of programs, strategies, and policies aimed to address root causes of public health problems at the individual, relationship, community, and societal levels (Runyan & Freire, 2007). Some of these efforts are similar to those traditionally used with gang violence, such as law enforcement strategies that involve policing and incarcerating gang-involved youth. However, public health widens the opportunities to intervene by attempting to prevent problems, like gang involvement and violence, before they begin. In public health, prevention programs are often structured in three categories, which relate to the group of interest (Dahlberg & Krug, 2002).
- Universal prevention programs are offered, regardless of risk for gang involvement or violence, to groups such as school-aged children.
- Selected prevention programs are aimed at children/youth considered at-risk for gang involvement or violence.
- Indicated prevention programs are aimed at children/youth who are already involved in gangs or gang violence.
Traditionally, gang prevention programs have focused on intervening at the individual level; however, the field of public health is increasing recognition of the need to intervene at the community and societal levels. The socio-ecological model, which was used to better understand the risk and protective factors related to gang violence, can also be used to guide intervention planning. This model outlines key levels of intervention, such as individual risks, dysfunctional relationships, and school or community issues that might exacerbate violence, and larger societal issues that contribute to violence, such as social and economic inequalities, marginalization of certain racial and ethnic groups, cultural attitudes on masculinity, and prevailing social norms on how to handle conflict. Traditionally, gang prevention programs have focused on intervening at the individual level (Klein & Maxson, 2006); however, the field of public health is increasing recognition of the need to intervene at the community and societal levels (CDC, 2009).
Universal Prevention Programs. Universal prevention programs may reduce problems, such as gang violence, but these programs may also reduce other negative health outcomes associated with gang involvement, such as substance abuse, high-risk sexual behavior, school dropout, early pregnancy and parenthood, family problems, and unstable employment (Krohn, Ward, Thornberry, Lizotte, & Chu, 2011). The Gang Resistance Education and Training (GREAT) Program is an example of a school-based, universal gang violence prevention curriculum aimed at middle school students (Esbensen, Peterson, Taylor, & Osgood, 2011; "Gang Resistance and Education Training Program," 2013). The lessons include the development of self-management skills, social skills, and drug abuse education. Law enforcement officers lead each lesson. While the first evaluation of the GREAT program reported no effect on gang membership or delinquency, the second evaluation with a revised curriculum found that students who received the program had 39% lower odds of gang membership compared to a control group (Esbensen et al., 2011).
Selected Prevention Programs. Nurses, especially those who provide well-child care, play an important role in screening and identifying families at risk and in need of intervention (Sidora-Arcoleo et al., 2010). The Nurse-Family Partnership (NFP) is an example of prevention program that targets a selected population of first-time, low-income mothers in order to provide prenatal and early childhood home visitation by nurses ("Nurse Family Partnership," 2013; Olds et al., 1998). The NFP emphasizes the social-ecological environment of the child and mother. A fifteen year follow up of a randomized controlled trial of NFP found home visitation reduced incidence of many of the child’s negative long-term outcomes, such as running away, arrests, convictions and violations of probation, and other health risks, such as lifetime sexual partners, cigarettes smoked per day, and days having consumed alcohol (Olds et al., 1998). Many of the reductions occurred among factors that are also risks associated with gang affiliation; thus, it is likely that NFP would also reduce gang affiliation and gang violence though it has never been specifically evaluated for those outcomes.
The Montreal Prevention Treatment Program (Tremblay, Masse, Pagani, & Vitaro, 1996) is another example of a prevention program that targets a selected population. This program was intended for disruptive boys in early elementary school (i.e., 7-9 years of age). The program included parent training (e.g., monitoring skills, positive reinforcement, effective punishment, family crisis management, and reading skills) and social skills training for the children (e.g., pro-social skills, and self-control skills) lead by university-trained professionals (Tremblay et al., 1996). The program duration was approximately two years with some families receiving as many as 47 sessions. When the participants were 15 years old, the group that received the Montreal Prevention Treatment Program was compared to a group receiving no treatment. The treatment group had statistically significant reductions in gang involvement, substance abuse, and self-reported delinquency (Tremblay et al., 1996). In terms of gang involvement, at 12 years of age, 3% of the participants in the Montreal Prevention Treatment Program were gang-involved compared to 20% in the group that was not treated (Tremblay et al., 1996). Therefore, this program was able to demonstrate that intensive intervention early in elementary school can reduce many problem behaviors through mid-adolescence.
Indicated prevention programs intervene with youth involved in gangs or gang violence in order to reduce their rates of gang violence, re-arrest, and possibly gang affiliation. Indicated Prevention Programs. Indicated prevention programs intervene with youth involved in gangs or gang violence in order to reduce their rates of gang violence, re-arrest, and possibly gang affiliation. Some of these indicated programs are hospital-based and, consequently, work with patients who are recovering in the hospital after an injury. These prevention programs are particularly important when addressing gang violence as the risk for retaliatory violence and hospital recidivism is high. In 2009, a national network of hospital-based violence intervention programs (NNHVIPs) was created ("The National Network of Hospital-Based Violence Intervention Programs," 2013). This network includes several programs that work with youth who are gang-involved.
The Wraparound Project at University of San Francisco/San Francisco General Hospital is one example of a indicated hospital-based prevention program (Smith, Dobbins, Evans, Balhotra, & Dicker, 2013). The Wraparound Project identifies youth (aged 10 to 30 years) with violence-related injuries who are at high-risk for recurrent injury and rehospitalization. The program provides these youth with case management services that vary in intensity by youth risk-level and need and lasts approximately six months to a year. The program uses the youth’s hospital experience to provide what they describe as a “teachable moment” where the patient’s first introduction to the program occurs at the bedside. Hospital nurses caring for patients who are potential candidates for the Wraparound Project are in the position to make sure that their patients are connected to this program and encourage their patients to utilize these services when they are discharged. The case management services include mental health services, vocational training, employment, school enrollment/GED, court advocacy, housing, substance abuse services. The rate of rehospitalization was examined for the time that the Wraparound Project has been in service (2005-2011). It was determined that this program decreased the rate of rehospitalization from 16% to 4.5% for youth at high risk of recurrent injury (Smith, Dobbins, Evans, Balhotra, & Dicker, 2013).
...prevention programs are particularly important when addressing gang violence as the risk for retaliatory violence and hospital recidivism is high. Cure Violence (also known as CeaseFire in Chicago or Safe Street in Baltimore) is an example of a prevention program targeting an indicated population that combines work at the community and individual level ("Cure Violence," 2013; Webster, Whitehill, Vernick, & Parker, 2012). At the community level, the program has sponsored media campaigns targeted at changing social norms related to violence. At the individual level, the program employs “violence interrupters” who are often former gang members who work in communities and hospitals to mediate conflict and prevent the escalation of retaliatory violence. These violence interrupters also work with, or act as, case managers. Several evaluations of the Cure Violence have been conducted in a number of cities. The Baltimore evaluation estimated that the program was associated with “5.4 fewer homicide incidents and 34.5 fewer nonfatal shooting incidents during 112 cumulative months of intervention post-observations”(Webster et al., 2012, p. 3).
...the therapist may provide support at the individual level by addressing the youth’s issues with impulsivity, at the family level by teaching parenting skills, and at the school level by working with the youth’s teachers to address the youth’s truancy. There are several promising programs for indicated populations that attempt to modify etiologic factors associated with gang affiliation and violence (Shute, 2013). These programs tend to be family-based with a strong emphasis on parent and youth skill-building. For example, Multisystemic Therapy (MST) is an evidence-based intervention that targets antisocial youth (aged 12-17 years) using a home-based, intensive family therapy (Henggeler, Cunningham, Pickrel, Schoenwald, & Brondino, 1996; "Multisystemic Therapy," 2013). MST is delivered by a therapist who develops a treatment plan that is individualized to the youth and their family, but considers the youth’s socio-ecological context and the etiology of antisocial behavior (Henggeler et al., 1996). For example, the therapist may provide support at the individual level by addressing the youth’s issues with impulsivity, at the family level by teaching parenting skills, and at the school level by working with the youth’s teachers to address the youth’s truancy. Rigorous evaluations of MST show reduction in offending, aggressive behavior and arrest, delinquent peer associations and improvements in parenting skills and family functioning. MST has been noted as a promising approach for gang affiliated youth (Shute, 2013) with some MST sites actively using MST with gang-involved youth.
Functional Family Therapy (FFT) shares many similarities with MST, but is even more family-focused and includes a phased-based treatment model ("Functional Family Therapy," 2013; Sexton & Turner, 2010). A recent randomized trial of FFT found that when FFT was practiced with model adherence there was a 35% reduction in felony crime and a 30% reduction in violent crimes when compared to a probation only group (Sexton & Turner, 2010). FFT has been disseminated to over 300 community settings in the U.S.; consequently, it has been used in a variety of settings with a diverse group of youth and their families (Sexton & Turner, 2010).
...sizable reductions in health problems, including gang violence, only results from broadly disseminating and implementing successful prevention programs or strategies. The field of public health is very cognizant that sizable reductions in health problems, including gang violence, only results from broadly disseminating and implementing successful prevention programs or strategies. Nurses play a critical role in disseminating health interventions. They are often able to break down medical science in a way that patients can easily understand. For example, they may provide their patients with information about risks and consequences of a health condition, explain intervention options that are available or provide referrals to prevention programs. Extending this type of health communication more broadly to problems such as gang violence will be critical to ensuring that this science reaches the populations most vulnerable to its effects.
As in each of the other steps of the public health model, there are a number of strategies employed to promote the dissemination of research into broad practice (Sogolow, Sleet, & Saul, 2007). Many strategies are directed at researchers who are developing interventions, such as the suggestion to involve the program’s target community in the planning and implementation of the intervention or to develop information for practitioners about what makes the program work (i.e., the core element and key program characteristics) so that program fidelity will be maintained.
OJJDP has developed a tool that provides a good example of one attempt to bridge the gap between gang research and practice. The tool includes three elements:
- OJJDP’s publication, A Guide to Assessing Your Community’s Youth Gang Problem (The National Gang Center, 2013b). This publication provides the information needed for communities to go from assessing their gang problem to reporting on their gang problem.
- OJJDP video on their comprehensive gang model (The National Gang Center, 2013a). This video reviews research on gang violence and provides tools for implementing gang prevention programs.
- OJJDP’s model programs guide (Development Services Group for the Office of Juvenile Justice and Delinquency Prevention, 2004) that provides information on gang prevention programs.
Conclusion
Prevention of complex societal problems, such as gang violence, requires substantial effort and sustained commitment from many sectors and disciplines. Having an understanding of the research on gang violence prevention will make nurses more equipped to help lead such efforts. Nurses historically have assumed the role as patient advocates by both protecting the rights of patients and encouraging promotion of well-being for their patients (Gaylord & Grace, 1995). Nurses can use the research available to inform decisions about gang violence prevention and to guide implementation of prevention strategies and thus reducing the health consequences of violence in their community. Nurses who provide care for gang-affiliated youth in hospitals may have the opportunity to refer their patients to community programs upon discharge. One challenge to this is that a national survey of nurses who work with adolescents has found that community resources for youth are not always available (Saewyc, Bearinger, McMahon, & Evans, 2006). More of the successful programs detailed above are needed.
...to date, no programs have been developed which attempt to prevent the formation of gangs. In addressing gang violence through a public health model, a number of critical challenges need to be considered. First, in regard to public health surveillance, the use of standardized definitions across disciplines will be important to monitoring the problem of gang violence. Second, a better understanding of the community- and society-level risks and protective factors will likely reveal new points of intervention. For example, to date, no programs have been developed which attempt to prevent the formation of gangs. Third, more attention needs to be placed on primary prevention programs that target gang involvement. Finally, there is a need for rigorous evaluation of programs for gang involved youth.
From developing a better understanding of patterns and causes of gang violence to knowing how to prevent youth from joining gangs in the first place, this article has offered a public health perspective of gang violence. Nurses who are interested in learning more about this topic can explore the sources of data, program descriptions, and online tools described to assist them to gather information to better understand gangs and gang violence. All nurses can be key players in finding solutions to the problem of gang violence and the field of public health, including public health nurses and other providors, is eager to support these efforts.
Note: The conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention
Acknowledgement
The authors want to acknowledge the National Institutes of Health, Eunice Kennedy Shriver National Institute of Child Health & Human Development for the grant K01-HD05798 (PI: Schneiderman) that supported the development of this manuscript. The content is solely the responsibility of the authors and does not necessarily represent the official views of National Institutes of Health or the Eunice Kennedy Shriver National Institute of Child Health & Human Development.
Authors
Dawn D. McDaniel, PhD
Email: Dawn.McDaniel@cdc.hhs.gov
Dawn McDaniel, PhD is currently a guest researcher in the Division of Violence Prevention at the Centers for Disease Control and Prevention (CDC) and a research psychologist at Virtually Better, Inc. She earned her Ph.D. in Clinical Psychology at the University of Southern California in Los Angeles, CA. Her research focuses on the prevention of gang violence, adolescent risk-taking, child maltreatment, and evidence-based interventions. She is also interested in novel uses of technology for solving complex public health problems. She completed a postdoctoral fellowship in applied epidemiology at the CDC and was a research scientist for the National Violent Death Reporting System. Her recent publications on this topic include Characteristics associated with gang homicide — five large cities, United States, 2003–2008; Risk and protective factors associated with gang affiliation among high risk youth: A public health approach; and Commitment language and homework completion in a behavioral employment program for gang-affiliated youth.
Joseph E. Logan, PhD
Email: ffa3@cdc.gov
Joseph Logan, PhD is a behavioral scientist in the Division of Violence Prevention at the Centers for Disease Control and Prevention (CDC). He earned his PhD at John Hopkins University in Baltimore, MD. His research focuses on using the public health perspective to gain a better understanding of violence for the purpose of improving prevention strategies. During his tenure at CDC, he has held the positions of Epidemic Intelligence Service (EIS) officer, EIS supervisor, and science officer for the National Violent Death Reporting System and the Youth Violence Prevention Centers. He conducts research in the areas of homicide, suicide, youth violence, child maltreatment, unintentional poisonings, mental health service research, and homicide-followed-by-suicide and has investigated multiple violence-related epidemics in the United States. His research has received numerous honors such as the MarketScan Investigator Award, the Alexander Langmuir Award, and multiple nominations for CDC’s Shepard Award.
Janet U. Schneiderman, PhD, RN
Email: juschnei@usc.edu
Janet U Schneiderman, PhD, MSN, BSN is a research associate professor at the University of Southern California in Los Angeles, CA. She earned her PhD in Education at USC. She taught public health and pediatric nursing at USC for 10 years from 1994 to 2004, before taking a faculty position at USC in the School of Social Work. Dr. Schneiderman has a K01 from the National Institutes of Health, Eunice Kennedy Shriver National Institute of Child Health & Human Development to study the prevention of medical neglect in the child welfare system. Dr. Schneiderman has been conducting research on the health and health care of abused and neglected children as well as other underserved youth. She, along with her colleagues, published one of the first public health nursing articles about gang youth as a vulnerable population. Her recent research has been targeted toward documenting the prevalence of obesity in children in foster care.
References
Boyle, D. J., & Hassett-Walker, C. (2008). Individual-level and socio-structural characteristics of violence: An emergency department study. Journal of Interpersonal Violence, 23(8), 1011-1026. doi: 10.1177/0886260507313966
Centers for Disease Control and Prevention. (2007). Web-based injury statistics query and reporting system (WISQUARS). Retrieved from www.cdc.gov/injury/wisqars/index.html
Centers for Disease Control and Prevention. (2009). CDC Injury Research Agenda, 2009-2018. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention.
Centers for Disease Control and Prevention. (2012). Gang homicides - five U.S. cities, 2003-2008. Morbidity and Mortality Weekly Report, 61(3), 46-51.
Changing course: Preventing gang membership. (2013). (T. Simon, N. Ritter & R. Mahendra Eds.). Washington, D.C.: U.S. Department of Justice, Office of Justice Programs, and the Centers for Disease Control and Prevention.
Cure violence. (2013). Retrieved from http://cureviolence.org
Dahlberg, L., & Krug, E. (2002). Violence, a global public health problem. In E. Krug, L. Dahlberg, J. Mercy, A. Zwi & R. Lozano (Eds.), World Report on Violence and Health. Geneva, Switzerland: World Health Organization.
Development Services Group for the Office of Juvenile Justice and Delinquency Prevention. (2004). Model programs guide. from www.ojjdp.gov/mpg/
Egley, A., Jr., & Howell, J. C. (2013). Highlights of the 2011 National Youth Gang Survey. Juvenile Justice Fact Sheet.
Esbensen, F.-A., Peterson, D., Taylor, T., & Osgood, D. (2011). Results from a multi-site evaluation of the G.R.E.A.T. program. Justice Quarterly, 29(1), 125-151. doi: 10.1080/07418825.2011.585995
Esbensen, F.-A., Winfree, L., He, N., & Taylor, T. (2001). Youth gangs and definitional issues: When is a gang a gang, and why does it matter? Crime & Delinquency, 47(1), 105.
The Eurogang Project. (2013). from www.umsl.edu/ccj/eurogang/euroganghome.html
Finkelhor, D., Turner, H., Ormrod, R., & Hamby, S. (2010). Trends in childhood violence and abuse exposure: Evidence from 2 national surveys. Archives of Pediatrics & Adolescent Medicine, 164(3), 238-242. doi: 10.1001/archpediatrics.2009.283
Functional family therapy. (2013). Retrieved from www.fftinc.com/
Gang Resistance and Education Training Program. (2013). Welcome to the G.R.E.A.T. web site. Retrieved from www.great-online.org/
Gaylord, N., & Grace, P. (1995). Nursing advocacy: An ethic of practice. Nursing ethics, 2(1), 11-18.
Glesmann, C., Krisberg, B., & Marchionna, S. (2009). Youth in gangs: Who is at risk? In National Council on Crime and Delinquency (Ed.), FOCUS. Oakland, CA.
Haegerich, T. M., Mercy, J., & Weiss, B. (2013). What is the role of public health in gang-membership prevention? . In T. Simon, N. Ritter & R. Mahendra (Eds.), Changing Course: Preventing Gang Membership. Washington, D.C.: U.S. Department of Justice, Office of Justice Programs, and the Centers for Disease Control and Prevention.
Harris, K. M., Halpern, C. T., Whitsel, E., Hussey, J., Tabor, J., Entzel, P., & Udry, J. R. (2009). The national longitudinal study of adolescent health: Research design. Retrieved from www.cpc.unc.edu/projects/addhealth/design
Henggeler, S. W., Cunningham, P. B., Pickrel, S. G., Schoenwald, S. K., & Brondino, M. J. (1996). Multisystemic therapy: An effective violence prevention approach for serious juvenile offenders. Journal of Adolescence, 19(1), 47-61.
Howell, J. C. (2012). Gangs in America's communities. Thousand Oaks: Sage.
Hutson, H., Anglin, D., Kyriacou, D., Hart, J., & Spears, K. (1995). The epidemic of gang-related homicides in Los Angeles County from 1979 through 1994. Journal of the American Medical Association, 274(13), 1031.
Karch, D. L., Logan, J., McDaniel, D., Parks, S., & Patel, N. (2012). Surveillance for violent deaths--National violent death reporting Ssystem, 16 states, 2009. Morbidity and Mortality Weekly Report: Surveillance Summaries, 61(6), 1-43.
Klein, M., & Maxson, C. (2006). Street gang patterns and policies. New York: Oxford University Press.
Krohn, M., Ward, J., Thornberry, T., Lizotte, A., & Chu, R. (2011). The cascading effects of adolescent gang involvement across the life course. Criminology, 49(4), 991-1028.
Lee, L. M., Thacker, S. B., & Louis, M. E. S. (2010). Principles & practice of public health surveillance. Oxford University Press, USA.
Marmot, M., Friel, S., Bell, R., Houweling, T. A. J., & Taylor, S. (2008). Closing the gap in a generation: Health equity through action on the social determinants of health. The Lancet, 372(9650), 1661-1669. doi: http://dx.doi.org/10.1016/S0140-6736(08)61690-6
Minnis, A. M., Moore, J. G., Doherty, I. A., Rodas, C., Auerswald, C., Shiboski, S., & Padian, N. S. (2008). Gang exposure and pregnancy incidence among female adolescents in San Francisco: Evidence for the need to integrate reproductive health with violence prevention efforts. American Journal of Epidemiology, 167(9), 1102-1109. doi: 10.1093/aje/kwn011
Multisystemic Therapy. (2013). What is multisystemic therapy? Retrieved from http://mstservices.com/
The National Gang Center. (2013a). About the national gang center. Retrieved from www.nationalgangcenter.gov
The National Gang Center. (2013b). OJJDP Comprehensive gang model online overview. Retrieved from www.nationalgangcenter.gov/Comprehensive-Gang-Model/Online-Overview
The National Gang Center. (2013c). Assessment guide. Retrieved from www.nationalgangcenter.gov/Comprehensive-Gang-Model/Assessment-Guide
The national network of hospital-based violence intervention programs. (2013). Retrieved from http://nnhvip.org/
Nurse family partnership. (2013). Retrieved from www.nursefamilypartnership.org
Olds, D., Henderson, C. R., Cole, R., Eckenrode, J., Kitzman, H., Luckey, D., . . . Powers, J. (1998). Long-term effects of nurse home visitation on children's criminal and antisocial behavior: 15-year follow-up of a randomized controlled trial. Journal of the American Medical Association, 280(14), 1238-1244. doi: 10.1001/jama.280.14.1238
Pyrooz, D. C. (2011). Structural covariates of gang homicide in large U.S. cities. Journal of Research in Crime and Delinquency, 48. doi: 10.1177/0022427811415535
Rosenberg, M. L., O'Carroll, P. W., & Powell, K. E. (1992). Let's be clear: Violence is a public health problem. Journal of the American Medical Association, 267(22), 3071-3072. doi: 10.1001/jama.1992.03480220089034
Runyan, C., & Freire, K. (2007). Developing interventions when there is little science. In L. Doll, S. Bonzo, J. Mercy, D. Sleet & E. Haas (Eds.), Handbook of injury and violence prevention (pp. 411-431). Atlanta, GA: Springer.
Saewyc, E. M., Bearinger, L. H., McMahon, G., & Evans, T. (2006). A national needs assessment of nurses providing health care to adolescents. Journal of Professional Nursing, 22(5), 304-313. doi: 10.1016/j.profnurs.2006.07.009
Sanders, B., Schneiderman, J. U., Loken, A., Lankenau, S. E., & Bloom, J. J. (2009). Gang youth as a vulnerable population for nursing intervention. Public Health Nursing, 26(4), 346-352. doi: 10.1111/j.1525-1446.2009.00789.x
Sexton, T., & Turner, C. W. (2010). The effectiveness of functional family therapy for youth with behavioral problems in a community practice setting. Journal of Family Psychology, 24(3), 339-348. doi: 10.1037/a0019406
Shute, J. (2013). Family support as a gang reduction measure. Children & Society, 27(1), 48-59.
Sidora-Arcoleo, K., Anson, E., Lorber, M., Cole, R., Olds, D., & Kitzman, H. (2010). Differential effects of a nurse home-visiting intervention on physically aggressive behavior in children. Journal of Pediatric Nursing, 25(1), 35-45. doi: http://dx.doi.org/10.1016/j.pedn.2008.07.011
Smith, R., Dobbins, S., Evans, A., Balhotra, K., & Dicker, R. A. (2013). Hospital-based violence intervention: Risk reduction resources that are essential for success. Journal of Trauma and Acute Care Surgery, 74(4), 976-982. doi: 10.1097/TA.0b013e31828586c9
Sogolow, E. D., Sleet, D. A., & Saul, J. (2007). Dissemination, implementation, and widespread use of injury prevention interventions. In L. Doll, S. Bonzo, J. Mercy, D. Sleet & E. Haas (Eds.), Handbook of injury and violence prevention (pp. 493-510). Atlanta, GA: Springer.
Tremblay, R., Masse, L., Pagani, L., & Vitaro, F. (1996). From childhood physical aggression to adolescent maladjustment: The Montreal prevention experiment. In R. D. Peters & R. J. McMahon (Eds.), Preventing childhood disorders, substance abuse, and delinquency (Vol. 3, pp. 268-298). Thousand Oaks: Sage.
Webster, D., Whitehill, J., Vernick, J., & Parker, E. (2012). Evaluation of Baltimore’s safe streets srograms: Effects on attitudes, participants’ experiences and gun violence. Baltimore, MD: Johns Hopkins Center for the Prevention of Youth Violence, Johns Hopkins Bloomberg School of Public Health.
Zeoli, A., Pizarro, J., Grady, S., & Melde, C. (2012). Homicide as infectious disease: Using public health methods to investigate the diffusion of homicide. Justice Quarterly, Published Online, 1-24. doi: 10.1080/07418825.2012.732100